The treatment of breast cancer is based upon several factors. Optimal management requires collaboration with breast surgeons and reconstructive or plastic surgeons, medical oncologists and radiation oncologists.
Early-stage localized breast cancer
Women with early stage breast cancer that has not spread beyond the breast need surgery. Two surgical options are available for treating localized breast cancer: mastectomy (removal of the breast) and breast-conserving therapy (removal of the cancerous tissue while preserving the non cancerous breast tissue).
We recognize that breast cancer surgery is a personal decision that can often be complex and overwhelming. Your care team will help you understand all your breast cancer surgery options, so you can decide on an individualized treatment plan tailored to you and your needs.
Mastectomy
This involves removal of the cancer and the surrounding normal breast tissue. This may cause cosmetic disfigurement and therefore breast reconstruction is needed along with a mastectomy. Radiation therapy to the chest wall and surrounding lymph node areas may also be needed after a mastectomy if the patient has a large tumor, positive lymph nodes, and positive surgical resection margins.
Breast-conserving therapy (BCT)
This is essentially designed to preserve the normal breast tissue so that the whole breast is not removed. BCT involves removal of the cancerous lump only by either a lumpectomy, wide excision, or partial mastectomy. BCT also requires radiation therapy to reduce the chances of recurrence of cancer in the same breast. The combination of surgery and radiation usually results in cosmetically acceptable preservation of the breast without compromising breast cancer outcomes. Up to two-thirds of patients with early breast cancer may be candidates for BCT. In general, survival outcomes are the same whether BCT or mastectomy is performed.
Breast reconstruction
This is an important option for women who undergo mastectomy. Breast reconstruction may be considered at the time of the mastectomy or at a later date. Consultation with a plastic surgeon prior to the mastectomy is essential if immediate reconstruction is desired. The need for postmastectomy radiation therapy may determine the timing of the reconstruction (immediate or delayed).
Adjuvant therapy
Anticancer treatment with drugs may be given before or after surgery. This is called “adjuvant systemic therapy.” The goal of adjuvant systemic therapy is to eliminate growth of any cancer cells that may have spread to other organs (metastases). The first site that breast cancer spreads to are the axillary lymph nodes (glands under the armpit). Presence of cancer in the lymph nodes lowers the chance for cure. Adjuvant systemic therapy is therefore important in this situation and improves overall survival.
There are three types of adjuvant systemic therapy. Patients may need one or more of these treatments depending on their tumor characteristics:
Hormonal therapy (endocrine or anti-estrogen treatment)
Hormonal therapy is only recommended for women with estrogen receptor (ER)-positive breast cancer. It has very few life-threatening side effects, is quite effective and therefore it is recommended for almost all women with ER-positive disease, regardless of stage. Endocrine therapy reduces the risk of breast cancer recurrence by 50 percent. There are two types of hormonal therapies that are used: selective estrogen receptor modulators (SERMs) such as tamoxifen or raloxifene, and aromatase inhibitors such as anastrozole.
Anti-HER2 therapy
Anti-HER2 therapy is usually recommended for patients whose tumours make a lot of HER2 protein. All breast cancer patients should have testing for the presence of HER2 protein in their cancer tissue that is removed during a biopsy of surgery.
Chemotherapy
The need for chemotherapy is based on many factors, such as the stage and grade of a tumor, presence of absence of hormone receptors and HER2 protein and the results of the 21 gene test (Oncotype DX). There are many types of chemotherapies and they are usually given in combination or in a sequential manner. The medical oncologist decides the regimen that is best for a particular situation. Sometimes, the medical oncologist may decide to give chemotherapy before surgery in some patients. This is known as neoadjuvant chemotherapy.

Locally advanced and inflammatory breast cancer
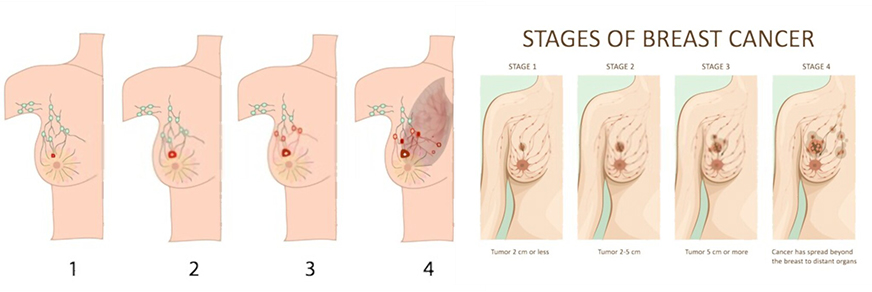
“Locally advanced breast cancer” usually implies one or more of the following: cancer larger than 5 cm, several enlarged surrounding lymph nodes, cancer nodules or ulceration in the skin overlying the breast, or fixation of the cancer to the chest wall behind the breast. Another form of locally advanced breast cancer is “inflammatory breast cancer,” which causes swelling, redness, or thickening of the skin due to its invasion by cancer cells. The likelihood of curing locally advanced and inflammatory breast cancer is lower than for smaller cancers.
Treatment generally includes a combination of chemotherapy, surgery, and radiation therapy. Additional therapies may include hormonal therapy (if the tumor is ER-positive) or trastuzumab (if the tumor is HER2 positive). In most cases, such therapy is given before surgery (called neoadjuvant therapy). At surgery, a larger proportion of patients are treated with mastectomy rather than breast conserving therapy (BCT). Almost all patients also need radiation therapy after surgery.

Metastatic breast cancer
Breast cancer patients in whom the cancer has spread to other organs (liver, lungs, bones) and distant lymph nodes need systemic therapy. Although a cure may not be possible, but therapy can prolong life, delay the progression of the cancer, relieve cancer-related symptoms, and improve quality of life. It is important to choose treatments that are more likely to reduce symptoms related to cancer with as few side effects as possible. A woman’s personal preferences are also very important to decide treatment in advanced cases. Surgery and radiation therapy may be needed to control disease in certain areas, such as painful bone metastases and skin metastases on the chest that are causing symptoms.
Read More – https://www.cancercenter.com/cancer-types/breast-cancer/treatments
Read More – https://www.breastcancer.org/treatment/radiation-therapy
What Our Patients Are Saying About Us

